Talk to Sales
Clinical Documentation Improvement (CDI): What It Is, Why It Matters, and What Modern Programs Actually Look Like
Poor clinical documentation doesn't just create compliance headaches — it costs hospitals real money. Inaccurate or incomplete records produce miscoded claims, trigger DRG downgrades, and hand payers grounds for denials that should never have occurred. Clinical documentation improvement (CDI) exists to close that gap: ensuring a patient's medical record captures the full clinical picture, so that the care delivered is accurately reflected in the codes submitted and the reimbursement received.
CDI programs have become a core function of the modern revenue cycle. The U.S. CDI market was valued at $2.5 billion in 2024 and is projected to reach nearly $4 billion by 2030. [Mordor Intelligence] That investment reflects the stakes: according to the 2024 MDaudit Benchmark Report, corrected inpatient claims can recover up to $4,900 per encounter, and the average health system has $11.2 million in at-risk revenue tied to coding inaccuracies at any given time. [MDaudit Benchmark Report 2024, via IKS Health]
What CDI Actually Does
At its core, CDI bridges the gap between the clinical narrative in a medical record and the coded data that drives reimbursement, quality reporting, and payer adjudication. When a physician documents "respiratory failure" without specifying type, laterality, or chronicity, a coder cannot assign the most accurate MS-DRG. When a comorbid condition like malnutrition or sepsis goes unaddressed in the documentation, the case gets grouped into a lower-weighted DRG than the patient's acuity warrants. CDI programs catch those gaps before the claim leaves the building.
The objectives are specific and financial:
Capturing the full severity of illness (SOI), complications and comorbidities (CCs), major CCs, and risk of mortality (ROM) ensures DRG assignment reflects what was actually delivered. Reducing denials tied to clinical validation — where payers challenge whether a queried diagnosis was adequately supported — requires defensible documentation before submission, not after. Improving quality metric scores for Hospital Acquired Conditions (HACs), Patient Safety Indicators (PSIs), and Social Determinants of Health (SDOH) reduces value-based penalties and strengthens performance benchmarks. And maintaining regulatory compliance means documentation functions as evidence of care, not just a billing record.
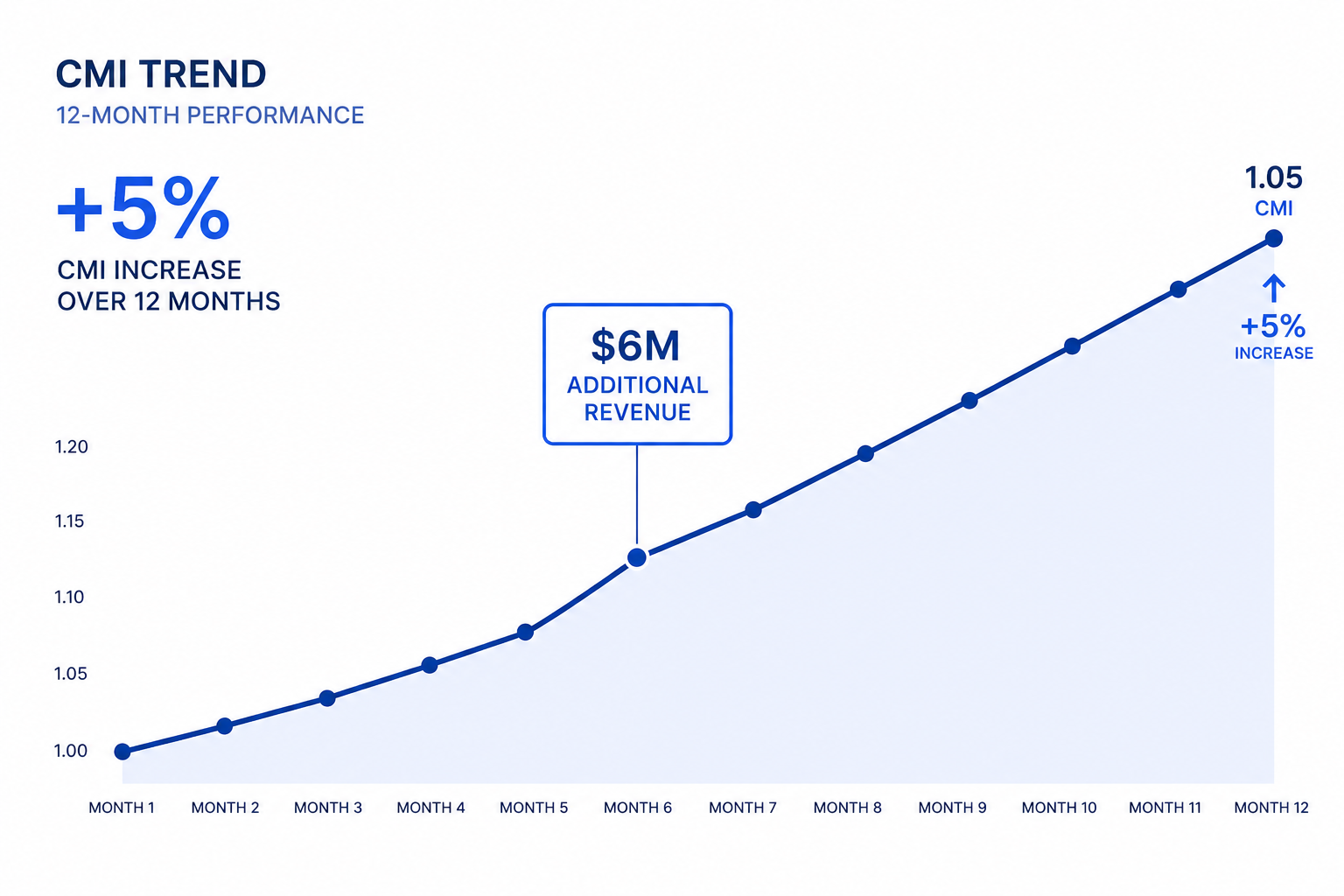
CDI programs that do this well see measurable CMI improvement. Structured CDI workflows supported by technology consistently produce a 3–8% Case Mix Index gain within 6–12 months of implementation. [CBS] For a hospital running 10,000 annual discharges at an average reimbursement of $12,000 per stay, a 5% CMI improvement translates to $6 million in additional annual revenue — from patients already being treated, without adding a single admission.
The CDI Specialist's Role
CDI specialists — typically registered nurses, advanced coders, or clinicians with HIM credentials — sit at the intersection of the clinical and coding worlds. Their job is to reduce documentation ambiguity before it becomes a coding problem and, ultimately, a denial.
The daily work involves concurrent chart review: identifying missing, unclear, or conflicting information that would compromise accurate DRG assignment. When gaps surface, specialists generate physician queries — structured clarification requests asking clinicians to confirm, expand, or correct documentation. Query compliance matters. According to 2024 ACDIS CDI Week survey data, 69% of organizations report physician query response rates between 91–100%, and roughly 49% see agree rates in that same range. [ACDIS] Those numbers reflect years of physician education and escalation infrastructure — not a given from program launch.
CDI specialists also validate CCs and MCCs against clinical indicators, review present-on-admission (POA) designations, and flag diagnoses likely to draw clinical validation denials from payers. The AHIMA/ACDIS joint guidelines on compliant query practice — last updated in 2022 with a denial-focused addendum in 2023 — establish the framework for this work. Queries must be grounded in legitimate clinical indicators, use non-leading language, and withstand payer scrutiny on appeal. [ACDIS/AHIMA Guidelines for Achieving a Compliant Query Practice, 2022 Update]
Cross-departmental reach is equally important. Effective CDI programs operate in coordination with Utilization Review (UR) for medical necessity documentation, Care Management for length-of-stay initiatives, HIM coding teams for DRG reconciliation and pre-bill review, and Finance for tracking clinical denial categories — DRG downgrades, clinical validation challenges, recoupments.
Where CDI Programs Break Down
The operational obstacles are consistent across organizations of every size.
Physician engagement remains the central challenge. Clinicians who view queries as administrative burden respond slowly or incompletely. Documentation education programs help, but require sustained investment and careful framing — CDI's value to clinicians must be presented as clinical support, not oversight.
Staffing constraints compound the problem. [American Hospital Association, 2026 Health Care Workforce Scan] CDI specialist shortages limit chart coverage, and when coverage drops, high-complexity cases slip through without review. Payer scrutiny makes this worse: as clinical validation denial rates climb, specialists spend more time defending individual claims in appeal workflows and less time performing concurrent review. The volume of work expands while the workforce doesn't.
AI integration introduces a different kind of pressure. New tools require governance policies, training, and workflow redesign before they deliver returns. Organizations adopting computer-assisted CDI without proper change management often see adoption friction that offsets the efficiency gains.
Finally, CDI programs face a measurement problem. Quantifying their financial contribution — attributing CMI shifts, denial reductions, and quality score improvements specifically to CDI activity — requires analytics infrastructure that many programs don't have. Without clear ROI visibility, CDI gets treated as overhead rather than revenue protection.
What AI and Technology Are Changing
The CDI software market claimed 66% of total CDI revenue in 2024 as providers shifted toward integrated, EHR-compatible platforms. [Mordor Intelligence] The capability profile of those platforms has changed significantly in the last two years.
Modern computer-assisted CDI tools use NLP and machine learning to analyze unstructured clinical notes in real time, extracting the clinical indicators a CDI specialist would look for — then surfacing query suggestions ranked by DRG impact. The review process that once required a specialist to open every chart now happens algorithmically, with human attention directed to the cases most likely to produce a meaningful outcome. AI-driven DRG prediction models now achieve an AUC of 0.88, with 41.8% of flagged cases generating DRG adjustments. [MDaudit]
Analytics capabilities have become equally important. CDI programs that feed performance data into dashboards — tracking CMI by service line and provider, CC/MCC capture rates, query response and agree rates, denial trend correlation — can shift from reactive chart review to targeted, data-driven physician education. Patterns that used to take quarters to identify now surface in weeks.
The integration layer matters too. Linking CDI platforms with computer-assisted coding (CAC) and computer-assisted professional coding (CAPC) creates a documentation-to-code pipeline that reduces audit risk, tightens DRG reconciliation, and enforces regulatory compliance across the claim lifecycle. Organizations running disconnected CDI and coding workflows are leaving both accuracy and revenue on the table.
The Expanding Scope of CDI
Inpatient programs still represent 62% of the CDI market by application setting, but that share is shrinking by design. [Mordor Intelligence] Outpatient CDI is projected to grow at a 9.46% CAGR through 2030 as payer scrutiny expands beyond acute care settings and value-based contracts begin applying documentation standards to ambulatory encounters, specialty practices, and post-acute facilities.
The same documentation principles that protect inpatient DRG assignment — specificity, comorbidity capture, clinical validation support — apply across every site of care. The programs that expand CDI beyond the hospital's four walls now will be better positioned when payers inevitably extend those standards.
Key Takeaways
A CDI program's financial impact is not theoretical. The revenue at stake — up to $4,900 per corrected inpatient claim, $11.2 million in coding-accuracy risk per organization — is recoverable through disciplined documentation improvement, accurate DRG capture, and denial prevention infrastructure. The technology to automate chart prioritization and surface query opportunities at scale exists and is proven. What separates high-performing CDI programs from struggling ones is not strategy — it's execution: physician engagement, cross-departmental integration, analytics visibility, and the right platform connecting it all.
ENTER's AI-powered RCM platform brings the same intelligence that drives CDI performance — real-time documentation analysis, denial trend visibility, coding accuracy monitoring, and workflow automation — to revenue cycle teams that need results without the operational overhead of building it from scratch. If your organization is looking to close documentation gaps and protect the revenue already being generated, visit enter.health to see what the platform can do.
Results
Sources
About the Author



ENTER is HIPAA compliant and SOC 2 Type 2 certified. See our trust center to learn more.