Talk to Sales
AI and A/R Automation in Healthcare: Fact or Fiction?
RCM leaders are being sold on "zero-touch claims," fully autonomous accounts receivable, and AI that makes billing staff obsolete. Meanwhile, most health systems are still fighting fragmented payer portals, inconsistent denial reason codes, and A/R backlogs that compound every quarter. The gap between the pitch and the reality is wide — and expensive if you build strategy around the wrong version.
AI and automation are genuinely reshaping healthcare A/R. Just not the way vendor demos suggest. Here are six reality checks that separate what works now from what remains future state.
Fact 1: Fully Autonomous A/R Is Not Right Around the Corner
The promise of a lights-out revenue cycle — where AI handles everything from claim submission to denial resolution without human input — makes for a compelling slide deck. It is not a near-term operational reality for most health systems.
What AI and automation actually do well today is reshape how A/R teams spend their time. RPA handles repetitive, rules-based tasks: claim status checks, portal navigation, data movement between systems. Intelligent routing prioritizes accounts by age, value, and risk without anyone touching a work queue. What does not automate cleanly is the judgment layer — interpreting payer behavior, resolving complex clinical denials, catching model drift before it affects collections.
The organizations seeing real gains are not chasing full autonomy. They are designing hybrid models where automated workflows handle volume and human staff focus on exceptions, governance, and the denial categories that require clinical or contractual expertise. That division of labor is what moves the needle on days in A/R.
What this means for RCM leaders: Design your automation architecture around the hybrid model, not the autonomous endpoint. The ROI is in the hybrid.
Fact 2: Zero-Touch Claims Work in Narrow Lanes
Electronic claim submission is largely automated. That part is true. But "zero touch" as a blanket operational target breaks down the moment you account for payer-specific attachment requirements, portal-based workflows that do not accept API calls, and the inconsistent application of denial reason codes across commercial payers.
Where straight-through processing delivers real value today is in defined, standardized workflows. Pre-submission scrubbing catches missing fields and obvious coding errors before a claim leaves the system. Automated claim status checks — via API or bot — replace manual portal navigation for high-volume, no-response follow-up. Payment posting and underpayment identification using contract models can run largely without human intervention.
Where it breaks down is payer variability. Variable adjudication logic, non-standard documentation requirements, and denial reason codes that mean different things at different payers make full automation unreliable in these lanes. Deploying automation there without human checkpoints creates the conditions for systematic write-offs.
What this means for RCM leaders: The right target is "maximum appropriate automation" per workflow — not zero human touch everywhere. Identify which steps are standardized enough to automate fully, and which need a human in the loop before the account ages further.
Fact 3: Bad Data Plus AI Equals Faster Failures
Deploying AI on top of a broken process does not fix the process. It scales the problem.
Before committing resources to any A/R automation initiative, three questions determine readiness. First: is the process standardized? If different staff handle the same denial type in three different ways, it is not ready for automation — it needs process design first. Second: is the task genuinely repetitive and rules-based? High-volume, rule-driven tasks with predictable inputs are automation candidates. Tasks where every account requires fresh judgment are not. Third: are the inputs digital and reliable? Paper, fax, and unstructured notes are not an AI-ready data foundation. Either build that foundation first or invest in extraction and normalization infrastructure capable of cleaning the data before it reaches any model.
A useful heuristic: if data is the primary driver of a decision, it is a candidate for automation. If expert knowledge is the primary driver, keep humans primary and use AI to support — not replace — that judgment.
What this means for RCM leaders: Process discipline and data quality determine automation ROI. AI amplifies whatever already exists in your operations. Make sure what exists is worth amplifying.
Fact 4: GenAI Wins in Targeted Denial Use Cases, Not as a Standalone Solution
Generative AI has genuine clinical and operational applications in denial management. The mistake is treating it as a denial robot that runs independently. The actual wins come from focused, measurable use cases where humans review outputs and governance structures are in place.
Next-best-action models that recommend whether to appeal, rebill, or adjust — based on payer behavior patterns, denial type, and propensity-to-overturn scores — reduce the cognitive load on denial specialists and surface the highest-recovery accounts first. GenAI-assisted appeal drafting generates first drafts for staff to review and refine, compressing the time from denial receipt to appeal submission. Analytics dashboards that surface denial patterns by payer, denial type, diagnosis code, and provider location turn reactive work into proactive prevention.
These are productivity tools for denial teams. They require ongoing prompt refinement, accuracy monitoring, and human review loops. What they are not: set-and-forget automation that eliminates the denial specialist role.
What this means for RCM leaders: Define specific, measurable use cases before selecting any GenAI tool. Monitor outcomes continuously. The productivity gains are real — but they require active governance, not passive deployment.
Fact 5: No Single Platform Solves A/R Automation
Any vendor claiming their platform will resolve your A/R automation challenges in one deployment is either misunderstanding your environment or oversimplifying theirs. Successful A/R automation is not a product purchase — it is an enterprise capability built over time with cross-functional ownership.
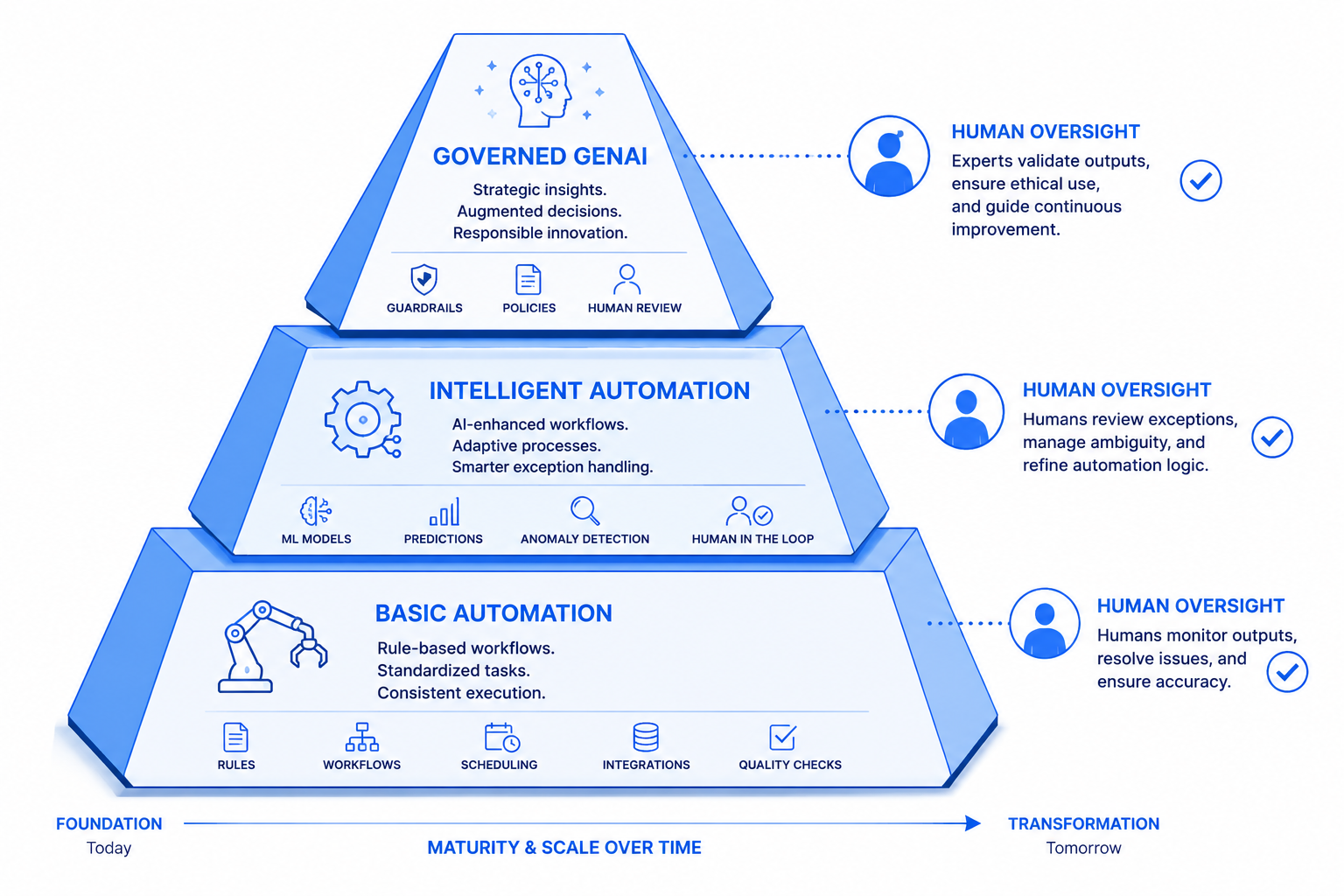
High-performing organizations treat automation as a phased program: basic automation first (RPA, status checks, payment posting), then intelligent automation (prioritization models, propensity scoring), then governed GenAI applied to denial drafting and appeal management. Each phase requires piloting in high-value, data-rich workflows before scaling. Each phase requires shared accountability across revenue cycle, IT, compliance, finance, and clinical stakeholders.
The CFO-level metrics that matter — A/R days, cost to collect, cash acceleration, write-off rate — should define success at every phase. "Tasks automated" is an input metric. Cash collected per FTE and net collection rate improvement are output metrics. Build reporting around the outputs.
What this means for RCM leaders: Ask prospective partners for real outcome data, including where implementations did not perform as expected. A partner who shares failure data alongside success data has a roadmap that will actually hold up.
Fact 6: The Biggest Risk Is Ungoverned Models, Not Moving Too Slowly
The argument for urgency in A/R automation is legitimate — payers have been deploying AI to deny claims faster, and organizations that do nothing will fall further behind. But the response to that pressure cannot be ungoverned deployment.
The most common failure modes in AI-driven A/R automation are not technical. They are operational and structural: models trained on biased or error-filled historical data; no pre/post performance baselines to measure impact; no clear accountability for model decisions; compliance and audit risk that was never formally assessed. The organizations that have had to unwind automation programs share a common thread — they moved fast and skipped governance.
Strong programs build governance in from the start: model approval processes, ongoing accuracy and bias monitoring, clear human-in-the-loop checkpoints at high-stakes decision points, and transparent metrics that connect automation activity to financial and operational outcomes. AI in a claims environment needs to be auditable and explainable. Regulators and payers will eventually require it. Building that infrastructure now is cheaper than retrofitting it under pressure.
What this means for RCM leaders: Speed without governance is not a competitive advantage. Build the accountability structure first, then accelerate.
Where to Start
The practical path forward combines prioritization with discipline. Identify two or three high-impact, data-rich workflows — no-response claims follow-up, specific denial types with high overturn rates, underpayment identification — and run structured pilots with clear success metrics. Align IT, revenue cycle, and compliance around a shared automation roadmap before selecting technology. Build the governance structure before scaling.
The organizations pulling ahead on A/R automation are not the ones with the most AI tools. They are the ones with the clearest frameworks for deciding where automation applies, the operational discipline to measure what changes, and the hybrid model that keeps human judgment in the loop where it matters most.
ENTER's platform is built for exactly this environment — combining AI-driven workflow automation, denial analytics, and payment intelligence in a system designed to integrate with your existing infrastructure. If you are building a roadmap for A/R automation, enter.health is a practical place to start.
Key Takeaways
- Hybrid human-plus-automation models outperform fully autonomous approaches in current A/R environments
- "Maximum appropriate automation" per workflow is a more useful target than zero-touch everywhere
- Data quality and process standardization determine automation ROI — AI scales what already exists
- GenAI in denial management works when scoped to specific use cases with active human oversight
- A/R automation is a phased program requiring cross-functional governance, not a single platform purchase
- Ungoverned models and unmeasured outcomes are higher-risk than moving deliberately
FAQ
What is A/R automation in healthcare revenue cycle management?
A/R automation in healthcare RCM uses RPA, AI, and intelligent routing to handle repetitive tasks in accounts receivable — claim status checks, payment posting, denial prioritization, and underpayment identification — without manual intervention at each step. The goal is to accelerate cash collection and reduce cost to collect while allowing staff to focus on complex, judgment-intensive work.
Can AI fully replace A/R staff in healthcare?
No. Current AI and automation tools work best in a hybrid model where automated workflows handle high-volume, rules-based tasks and human staff manage exceptions, complex denials, and governance oversight. Fully autonomous A/R remains future state for most organizations.
Which A/R workflows are most ready for automation?
Pre-submission claim scrubbing, automated claim status checks via API or RPA, payment posting, and underpayment identification using contract models are the workflows most consistently delivering results at scale. Workflows with high payer variability or non-standard documentation requirements require more human oversight.
What role does generative AI play in denial management?
GenAI supports denial management through next-best-action recommendations, propensity-to-overturn scoring, and first-draft appeal letter generation. These are productivity tools that require active human review and governance — not autonomous denial resolution.
What governance structures does AI-driven A/R automation require?
Effective governance includes model approval and change control processes, ongoing accuracy and bias monitoring, pre/post performance baselines, human-in-the-loop checkpoints at high-stakes decision points, and transparent metrics connecting automation activity to financial outcomes like A/R days and net collection rate.
Results
Sources
About the Author



ENTER is HIPAA compliant and SOC 2 Type 2 certified. See our trust center to learn more.