Talk to Sales
How Payment Posting Accuracy Can Cost Practices Thousands

Payment posting errors don't announce themselves. They accumulate quietly — a transposed digit here, a generic adjustment code there — until the damage shows up in your accounts receivable aging report, your denial rate, or a patient complaint. By then, the money is already gone.
The loss comes from two directions simultaneously: you pay staff to do work that machines handle better, and the errors those staff members make allow insurance underpayments and missed charges to slip through undetected. Both erode margin. Neither is inevitable.
What Payment Posting Actually Does
Payment posting is the process of recording money received from insurers and patients against the corresponding claims. When an insurance company pays a claim, it sends either a paper Explanation of Benefits (EOB) or an Electronic Remittance Advice (ERA). Your billing team takes that document — however it arrives — matches each payment line to the right claim, applies the contractual write-offs, and updates the remaining patient balance.
The complexity lies in the "however it arrives" part. Some payments come as paper checks with paper EOBs. Others download automatically as ERA files into your practice management system. Still others require logging into insurer portals to pull PDFs manually. Each channel demands different handling, and each is a separate opportunity for error.
HFMA's 2024 "Curing Payment Confusion" report found that 83% of healthcare finance leaders believe their organizations explain financial matters clearly to patients — yet a persistent gap exists between what providers perceive and what patients actually experience. Accurate payment posting is the foundation under that gap.
The Real Cost of Manual Posting
The labor expense alone justifies attention. MGMA's 2023 Cost Survey found that staffing accounts for 45–60% of total practice operating costs, with billing and collections staff representing a significant share.
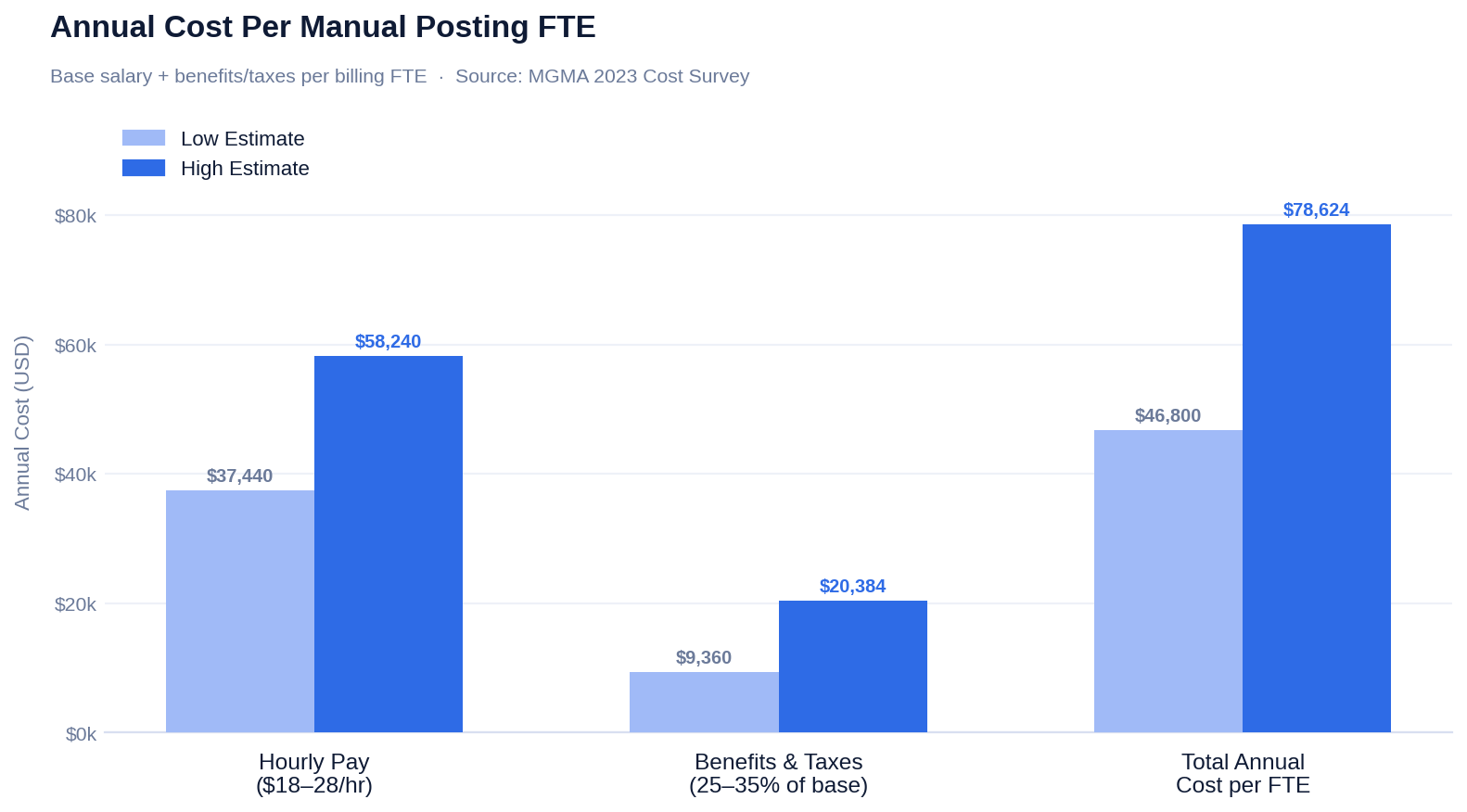
That's the floor. It doesn't count the revenue lost when that employee makes a mistake.
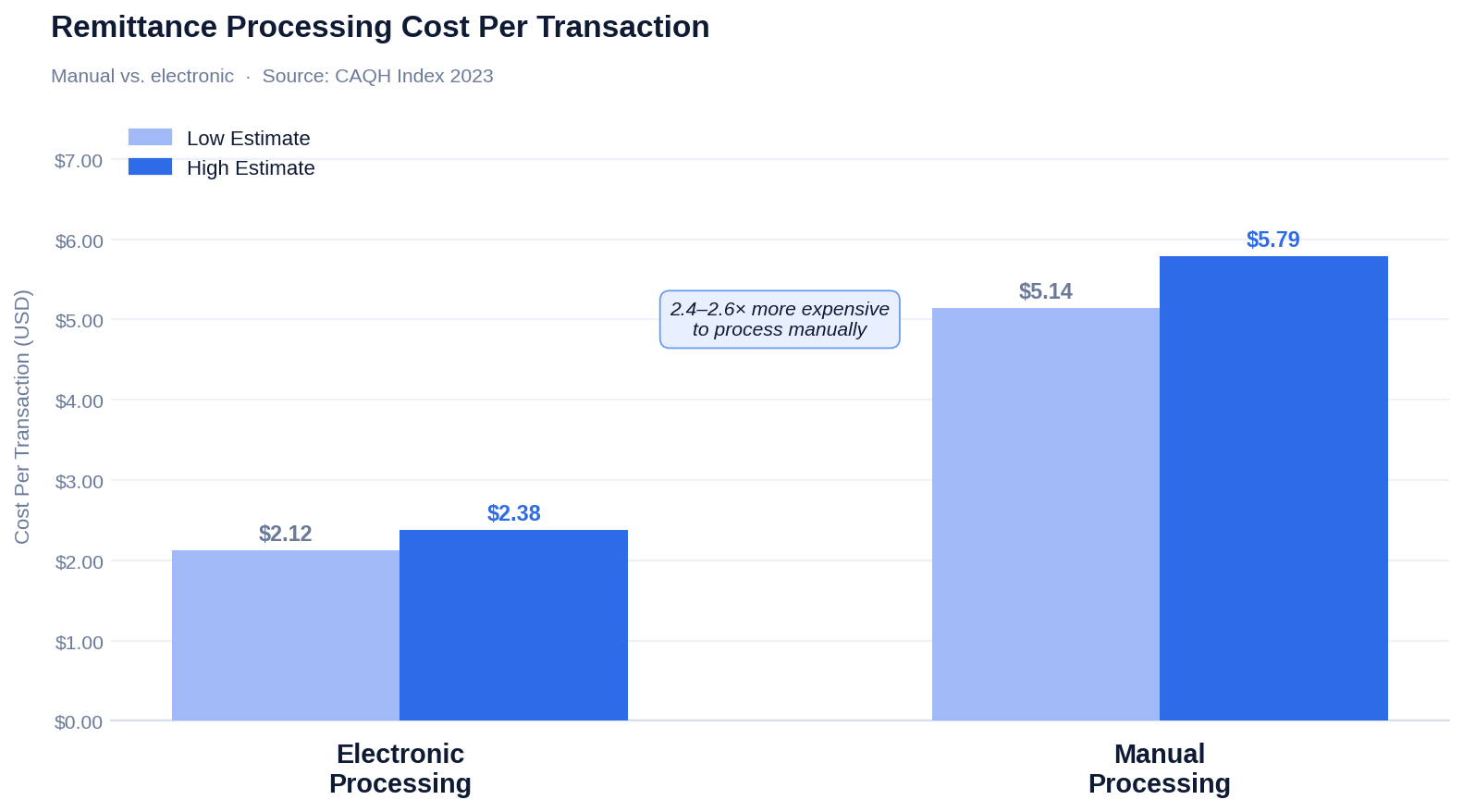
For context on what automation saves: the 2023 CAQH Index puts electronic remittance processing at $2.12–$2.38 per transaction versus $5.14–$5.79 for fully manual processing. Across thousands of transactions monthly, the difference is not marginal.
What Posting Errors Actually Do to Your Revenue
A staff member receives a payment for $100.10 and enters $10,010. The patient now shows a $10,010 credit. The practice almost certainly never collects what that patient actually owes. The patient gets a bill that makes no sense and calls to dispute it. A staff member stops doing productive work to investigate and fix the error.
That's one mistake. In a high-volume practice, small error rates compound into tens of thousands in annual losses.
Common failure modes include:
Accidentally writing off a claim as a contractual adjustment and never collecting the balance. Patient accounts reflecting balances already paid, triggering disputes. Denial management work halted while staff investigate posting errors. Appeal windows closing before the error is caught and the correct claim resubmitted.
HFMA data shows initial claim denial rates reached nearly 12% in 2024 — up 2.4% year over year. Separately, research shows 85% of those denials are avoidable. And HFMA reports that 42% of denials trace back to coding issues — the exact category where inaccurate adjustment coding creates the most damage.
Why Adjustments Are Where Money Disappears
Adjustments are the category most likely to conceal losses. When staff are under pressure to hit daily posting quotas, the path of least resistance is applying a generic code — typically CO-45 (contractual adjustment) — and moving on. The numbers balance. The problem disappears from view. The underpayment stays.
The downstream effects are structural. Without granular adjustment data, you cannot see which insurers consistently underpay for specific procedure codes, which denial reasons recur month after month, or which credentialing gaps are blocking payment for individual providers. You're flying blind during contract negotiations and unable to build a meaningful denial prevention strategy.
The difference between generic tracking and real tracking is measurable:
CMS-1500 compliance guidelines require detailed adjustment tracking for Medicare audit trail purposes. A denial for "missing information" demands a different correction than a denial for "service not covered." Without clean tracking, audits become difficult and compliance gaps accumulate without anyone noticing.
What Automation Fixes
Automated payment posting software reads ERA files and enters payment data directly into your system. No manual typing. No transposition errors. Payments post in minutes rather than days, and accounts reflect current balances in real time.
The operational impact extends beyond accuracy. When posting is automated, your RCM team stops functioning as data entry staff and starts functioning as revenue recovery specialists. They analyze denial patterns, appeal underpayments, contact patients about overdue balances, and identify contract performance problems — work that actually grows revenue rather than just recording it.
The 2023 CAQH Index found that electronic remittance advice adoption reached 88% across the medical industry — the largest single-year increase among all tracked transactions. Fully automated end-to-end posting, however, remains inconsistently implemented. That gap is where practices continue to lose money.
ENTER's AI-powered RCM platform validates each adjustment automatically against payer contracts, flagging discrepancies before they become write-offs.
What Real-Time Posting Does for Cash Flow
When payments post daily with high accuracy, your billing team operates on current information. They stop calling insurers about claims already paid. They catch underpayments before appeal windows close. They see denial patterns within days instead of discovering them at month-end.
HFMA reports that the average administrative cost to rework a Medicare Advantage denial is $47.77, and $63.76 for a commercial denial. Clean, accurate posting doesn't just prevent errors — it prevents the downstream rework cost that compounds them.
Top-performing practices hit benchmarks that manual posting makes difficult to sustain:
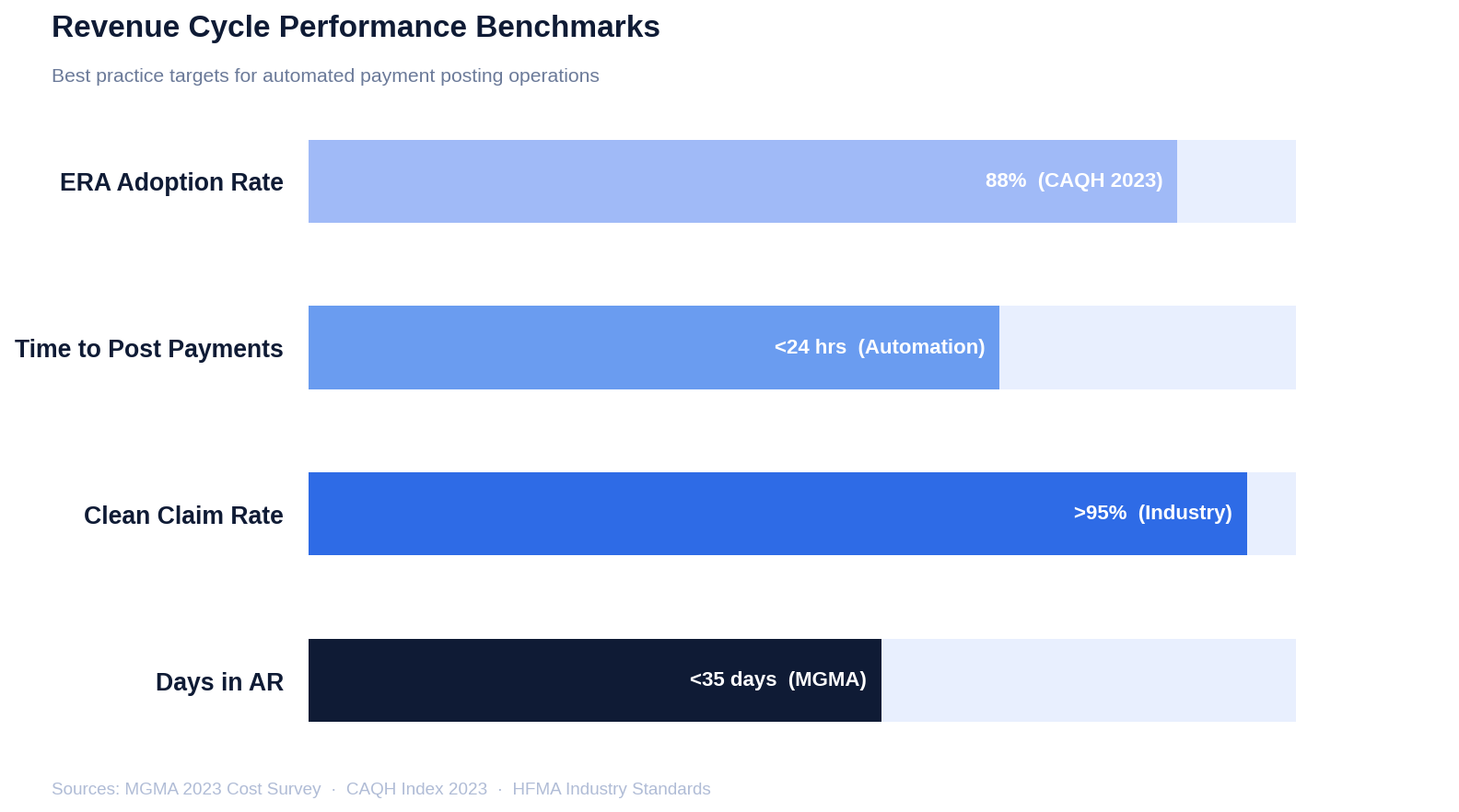
Every day of reduction in AR days accelerates cash flow directly. The math is simple: faster posting means faster visibility, which means faster intervention when something is wrong.
What a Real Adjustment Tracking System Looks Like
A functional adjustment tracking system categorizes every dollar not collected, assigns the correct reason code, maps it to the responsible payer, and surfaces patterns. The minimum requirements:
Automated ERA parsing — reads insurance payment files and maps data directly to claims without manual re-entry.
Standardized adjustment coding — clear, consistent codes for every adjustment type, mapped to standard reason codes rather than whatever is convenient in the moment.
Payer performance reporting — denial rates by reason, payment amounts versus contracted rates, and time-to-payment by payer.
Pattern detection alerts — notifications when a denial reason exceeds threshold frequency, so problems get addressed before they become endemic.
Audit-ready documentation — complete records of every adjustment for OIG Work Plan compliance and MAC audit purposes.
ENTER's AI REST APIs integrate directly with existing practice management systems, automating data flow without requiring platform changes or staff retraining. When the data is clean and current, billing managers can identify the highest-frequency denials and address root causes. Leadership sees actual revenue performance rather than a lagged approximation of it.
Good tracking provides that transparency without creating additional work. That's the standard worth holding to.
Frequently Asked Questions
Why do insurance payments sometimes arrive for different amounts than expected?
Insurance companies pay based on your contracted rates, not what you billed. Your posting team should verify that the EOB reflects contractual adjustments correctly. If the paid amount doesn't match your contract, you may be looking at a denial, a bundling issue, or an outright underpayment that warrants an appeal.
How do I know if a denied claim was posted correctly?
Pull the claim in your AR report. If the denial posted correctly, the claim shows a zero balance with the appropriate denial code attached. If it still shows as unpaid with no denial code, someone needs to correct the posting before the appeal window closes.
What do negative balances in billing software mean?
Credit balances indicate a payment posted twice, an overpayment was received, or an adjustment was coded incorrectly. Run credit balance reports monthly and issue refunds when owed. Letting credit balances accumulate creates both compliance exposure and patient trust problems.
What happens to payments that arrive without a matching claim?
Park them in an unapplied cash account until you identify the correct claim. Contact the insurer for the missing EOB. Never apply payments without matching them to a specific claim — posting to the wrong account creates exactly the kind of cascading errors that take hours to unwind.
How does secondary insurance affect cash flow?
Secondary payments depend on primary insurance processing first, which delays final resolution. Your team needs to post both payments accurately to clear patient responsibility and avoid billing patients for amounts already covered. Delays in secondary posting are a common source of unnecessary patient-responsibility statements.
Accurate Posting Is a Revenue Decision
The math on payment posting accuracy isn't abstract. You pay staff to enter data, those staff make errors, and those errors either cost you revenue directly or generate rework that costs you time. Neither is recoverable without a process change.
ENTER's AI-powered platform eliminates manual posting errors, validates adjustments against payer contracts automatically, and integrates with your existing EHR and practice management system without a platform migration. The result is cleaner data, fewer write-offs, and an RCM team that spends its time on work that actually moves money — not work that just records it.
If your posting process is still manual, the question isn't whether it's costing you money. It's how much.
Results
Sources
About the Author



ENTER is HIPAA compliant and SOC 2 Type 2 certified. See our trust center to learn more.