Talk to Sales
2026 EMR Integration Costs for Medical Practices

The first quote looks reasonable. Then the project starts.
Interface mapping takes longer than anyone budgeted. The lab system needs its own connection. So does the pharmacy network. And the telehealth platform. Each one requires setup, testing, and compliance validation — and none of that was in the original number. Budgets that started near $20,000 routinely end up north of $100,000 by the time a practice goes live.
This isn't an exception. In fact, it's actually the rule. And it happens because the real cost of EMR integration is more than just the software, it's everything the software has to talk to.
Here's what practices actually pay, where the money goes, and how modern platforms are starting to change the math.
What EMR Integration Actually Costs in 2026
Most EMR integration projects fall somewhere between $15,000 and $200,000, according to KLAS Research data cited in a 2025 Healthcare IT News report. For large organizations running Epic or Oracle Cerner, that range extends to $165,000–$335,000 once you account for interface work, testing, and compliance overhead.
Those numbers assume you know what you're connecting. Many practices don't, at first.
A functioning EMR needs to exchange data with billing platforms, clearinghouses, lab systems, imaging archives, pharmacy networks, patient portals, and telehealth tools. Each of those connections is its own project: its own mapping work, its own testing cycles, its own maintenance burden. The ONC's 2024 Interoperability Report found that making disparate systems communicate reliably often becomes the single largest cost driver in an EMR implementation, ultimately outpacing the software license itself.
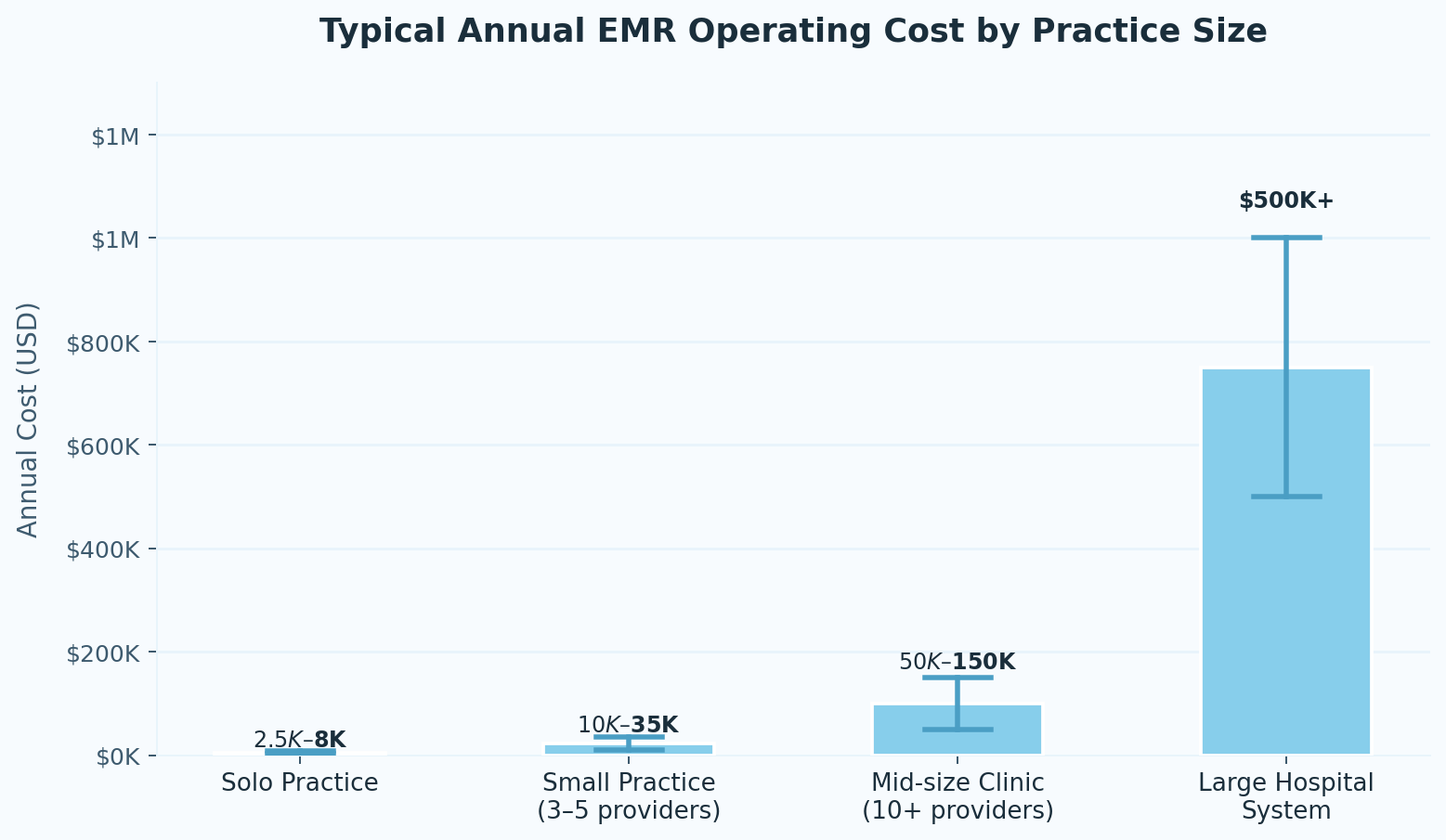
The table below shows what practices typically spend on an ongoing basis once integration, support, and upkeep are factored in:
Where the Budget Actually Goes
The line items that blow up EMR projects aren't mysterious, however. They're just easy to underestimate until you're in the middle of them.
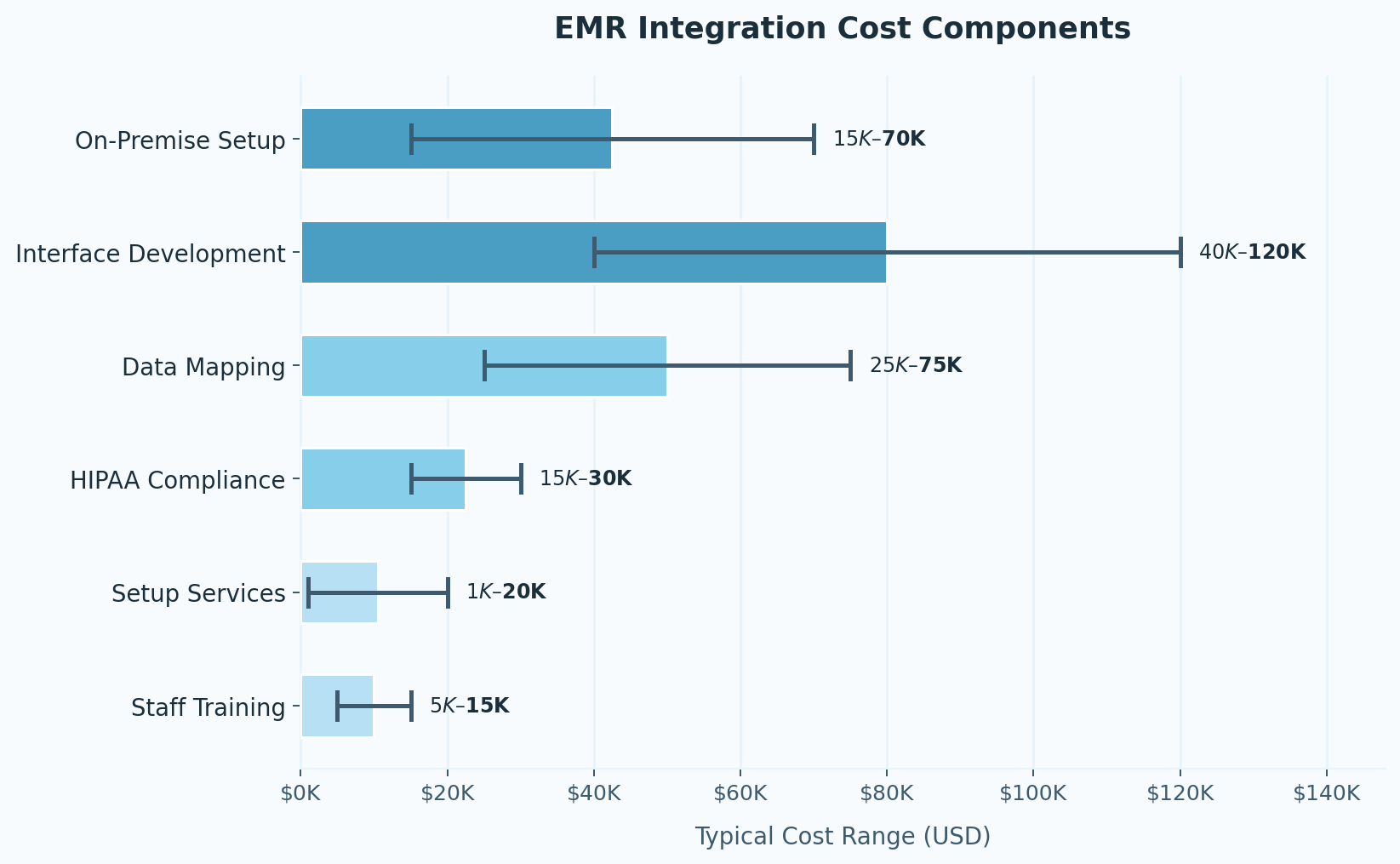
Interface work and data mapping are the biggest drivers, typically running $40,000–$120,000 for interface development and $25,000–$75,000 for data mapping depending on system complexity. Data doesn't move between systems automatically. Every field has to be mapped: patient ID, test code, result value, unit of measure, timestamp,and both systems have to read it the same way. For large systems with thousands of clinical data fields, this is months of work.
HIPAA compliance and security validation add another $15,000–$30,000. This goes beyondoptional overhead. It's a precondition for going live, and skipping it isn't actually an option.
The base software license is where most practices focus their attention, and where they underestimate least. Cloud-based EMR subscriptions typically run $200–$700 per provider per month, per Capterra's 2025 EMR Pricing Study. On-premise systems cost $15,000–$70,000 upfront with 15–20% annual maintenance on top of that.
Setup, configuration, and training are the line items that disappear from early estimates and reappear on final invoices. Setting up user roles, building clinical templates, configuring workflows — the ONC's 2024 Health IT Implementation Report notes that these tasks are chronically underestimated. Budget $1,000–$20,000 for setup services and $5,000–$15,000 for staff training as a starting point.
A 2024 KPMG report found that medical practices routinely underestimate initial implementation costs by 20–30%, primarily due to overlooked IT and workforce expenses. MGMA data from 2025 puts the problem in starker terms: operating expenses rose 11.1% year-over-year, with IT and cybersecurity among the largest contributors.
The Hidden Costs No One Puts in the First Quote
Beyond setup, there's a layer of ongoing costs that practices rarely budget for in advance.
System downtime is the one that stings most immediately. When an EMR goes down, billing stops. Staff can't work. The Ponemon Institute's 2025 Cost of Healthcare Data Breaches report estimates outages run $2,300–$8,600 per day in lost productivity and revenue. A single bad week can cost more than a year of integration maintenance.
Vendor overage charges appear when contracted support hours run out — which they will, especially in the first year. Be sure to read the fine print on support contracts before you sign!
API maintenance fees are the quiet ongoing cost of keeping system integrations functional as software updates roll out on both ends. Integrations that worked at launch need tending.
Security audits recur on a cadence, not just at go-live. HHS Office for Civil Rights penalties for serious HIPAA breaches can reach millions — the audit cost is not the problem; the alternative is.
Staff productivity loss during transition is real and measurable. Most practices see a 10–20% dip in the first few months as clinical and billing teams adjust. Plan for it explicitly rather than hoping it won't happen.
In October 2025, MGMA surveyed medical group leaders and found that for 30% of respondents, health IT — specifically EHR modernization and interoperability — had become the single largest new line item in their annual budget. That's not a technology trend. That's an operational reality.
Scale Doesn't Save You as Much as You Think
Larger organizations spread integration costs across more providers, which reduces the per-user number. A hospital system integrating Epic across hundreds of providers will pay less per clinician than a small clinic connecting the same platform. That math is real.
What doesn't scale down as cleanly: compliance requirements, cybersecurity obligations, multi-site interoperability complexity, and the internal IT staffing needed to manage it all. Enterprise networks carry significant fixed overhead that mid-size practices often underestimate when they look at enterprise pricing.
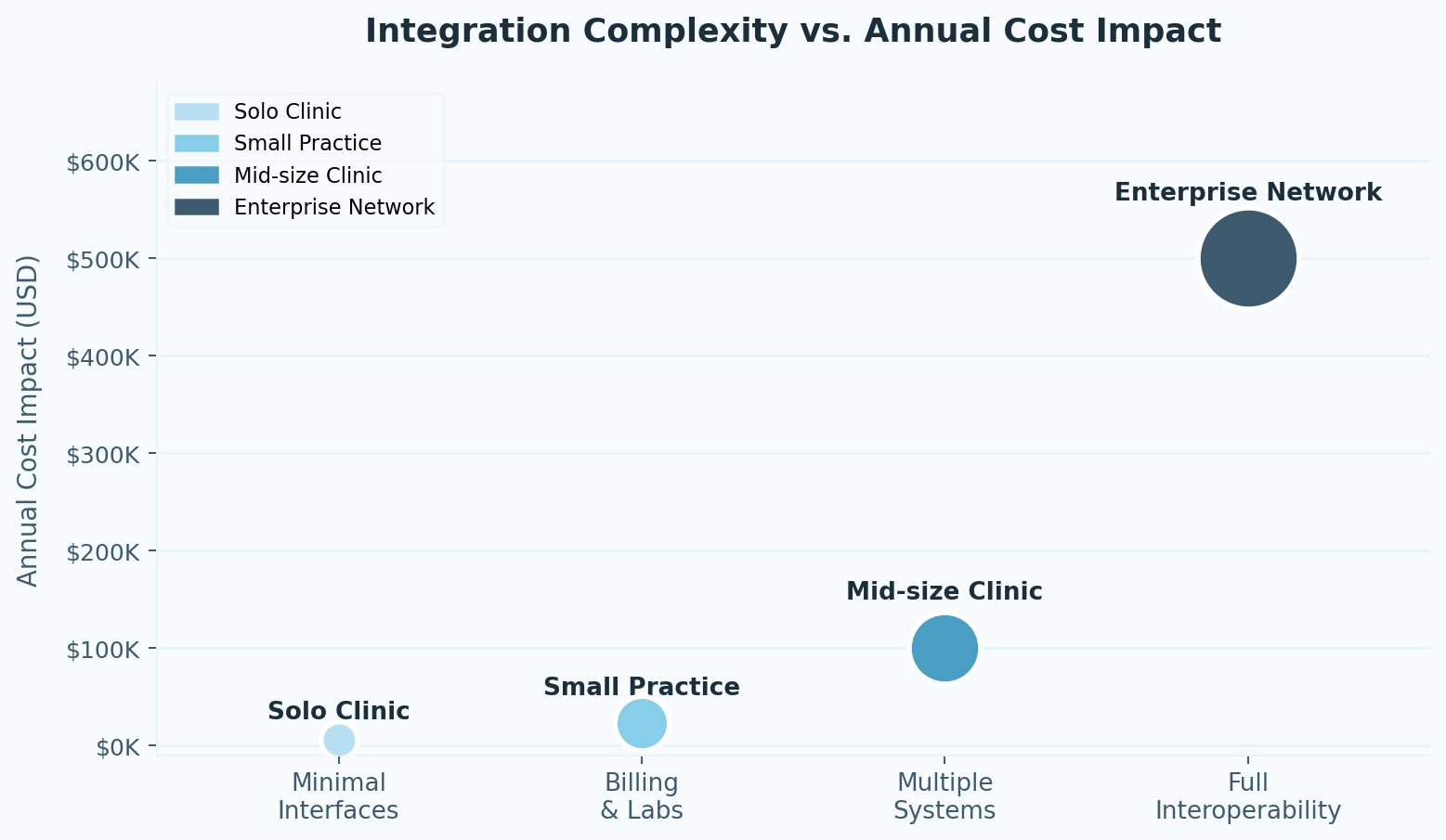
The more important question for growing organizations isn't what integration costs today — it's whether the system you're choosing can scale without requiring a full re-implementation when you add locations, analytics platforms, or value-based care reporting requirements two years from now.
What IT Teams See That Quotes Don't Show
The people who actually run EMR migrations are consistent about one thing: time is the budget killer, not software.
Data migration always surfaces surprises. Records that looked clean in the old system aren't. Field mappings that seemed straightforward need manual adjudication. Testing cycles that were supposed to take two weeks take six. Each fix requires another round of validation.
Vendor contracts regularly contain fees for system connections that weren't disclosed upfront. Consultant hours expand as project scope grows. And the final step — getting clinical and billing staff to sign off that the system actually works for their daily tasks — routinely becomes the last significant delay before launch.
The result: large implementations that were estimated at six months often run 12–18. The timeline extension is the cost extension.
How AI Is Starting to Change the Equation
The traditional integration model requires consultants to manually match data fields between systems, build connections one at a time, and run exhaustive test cycles to catch errors before go-live. It's slow, expensive, and scales poorly.
AI-powered platforms are replacing significant portions of that manual work. Machine learning can analyze existing data structures and suggest field mappings automatically. Automated testing tools can simulate thousands of transactions to catch errors before they reach production. And predictive error detection flags potential issues before they cause downstream problems in billing or clinical documentation.
For revenue cycle operations specifically, this matters beyond implementation. When claims data flows cleanly between clinical notes, billing systems, and clearinghouses — without manual intervention at each handoff — denial rates drop, clean claims move faster, and financial visibility improves. ENTER's ClaimAI is built around this principle: automation that doesn't just speed up the process but makes the underlying data reliable enough that the process can largely run itself.
That's where "get paid more, faster, with clear visibility" stops being positioning and becomes an operational description.
The Bottom Line
EMR integration that's priced only on the initial quote almost always ends in frustration — broken data flow, slow claims, staff hours spent on errors that shouldn't exist. The costs grow because the scope was never fully defined to begin with.
The practices that come out ahead are the ones that go in with a realistic picture of total cost of ownership: interface work, compliance overhead, staff transition time, and ongoing maintenance — not just the license fee.
ENTER works with healthcare organizations that want integration to actually function inside daily operations, not just pass go-live. When systems communicate reliably, claims process faster, reporting gets cleaner, and the revenue cycle starts to feel like infrastructure instead of a constant problem to manage.
Frequently Asked Questions
How will EMR integration change daily operations?
The immediate impact is usually reduced administrative burden. Lab results flow directly into patient records. Billing data moves automatically rather than being re-entered. The first two months typically involve a productivity dip while staff adjust; after that, well-implemented systems save measurable time across clinical and billing workflows.
What costs should I budget for after year one?
Annual support contracts typically run 15–20% of initial implementation costs. Plan for software update compatibility work, ongoing API maintenance as connected systems update, and new staff training as your team turns over. These aren't exceptional costs — they're the ongoing cost of operating integrated software.
How does connecting to external healthcare systems affect budget?
External connections — referral networks, hospital systems, specialty practices — require additional interface work and interoperability testing. The upfront cost is real. The long-term payoff is staff time saved chasing records, and more complete clinical data at the point of care.
How long until the team is fully up to speed?
Most practices reach operational fluency within two months. Having designated super-users on staff — people who learn the system first and support their colleagues — consistently shortens that timeline. Strong vendor support during the transition period matters more than most practices expect when they're evaluating vendors.
Results
Sources
About the Author



ENTER is HIPAA compliant and SOC 2 Type 2 certified. See our trust center to learn more.